DeBe: AI-enabled diabetes management
Connected Health Ecosystem for Diabetes Management
In Brief
Self-initiated venture, no client brief.
Six diabetes signals, no platform synthesises them all.
Concept: unified AI recommendation layer across all six.
AI-enhanced design, AI-enabled journeys.
Led end-to-end: research to go-to-market planning.
Synthetic patient modelling for quantitative depth.
Validated competitive gap across clinical literature.
Four-phase go-to-market roadmap.
Outcomes and Impact
This project is in progress; outcomes at this stage are methodological proof points, not commercial results.
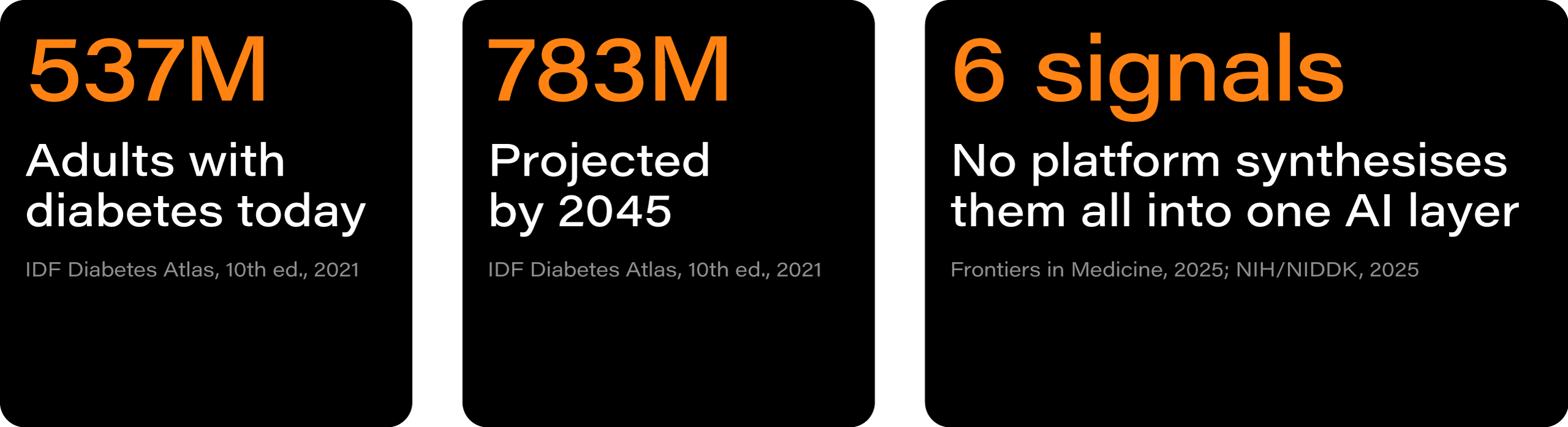
537M adults with diabetes globally.
6 health signals, no platform synthesises them all.
4 phases from research to public release.
0 deployed systems with a unified AI recommendation layer across all six signals.
Situation
Diabetes is manageable. But the tools to manage it are not.
The tools to manage diabetes exist. CGMs, fitness trackers, nutrition apps, blood pressure monitors. But they were built in isolation. They do not talk to each other. They do not think.
The entire responsibility of interpretation sits with the patient. Every correlation, every behaviour adjustment, every clinical decision is manual. For most people, that is not sustainable.
No existing platform integrates all six diabetes-relevant health signals simultaneously into a unified AI recommendation layer. The closest competitor integrates five. Blood oxygen is absent from every patient-facing product currently deployed. The barrier is structural: fragmented data standards, closed device ecosystems, no shared intelligence across sources.
This is a self-initiated project.
No client commissioned it.
The brief came from the problem itself.
Approach
Six diabetic signals. No system that makes sense of them.
AI compressed weeks of desk research into days. That changed what was possible at the start, when the strategic choices were still open and the problem was still forming.
The competitive landscape was validated across clinical literature, market reports, and platform data before a single design decision was made. Synthetic patient modelling added quantitative depth, simulating population-scale behaviour patterns and clinical edge cases where real recruitment would be too slow. Qualitative depth interviews with long-term patients provided the human signal no model can replace.
Two behavioural segments emerged. The Finders are newly diagnosed patients, still forming habits, looking for structure. The Fixers are long-term patients who know exactly where the current tools fail. Launch focus is the Fixers: faster validation, denser signal, clearer evidence base.
Regulatory obligations across GDPR, AI Act, EAA, and DSA/DMA were mapped from the start and embedded into the design system.
AI ran through every stage of this work, but at two distinct levels. As a strategic capability, it accelerated the thinking before any design decisions were made. As a product decision, it became the operating logic of the service itself: the mechanism that connects six signals, surfaces patterns, and generates actions the patient can trust.
Keeping those two roles distinct was one of the more consequential design choices in this project.
AI ran through every stage of this work, but at two distinct levels: as a strategic design capability and as a product logic.
AI-enhanced strategy & design
AI accelerates the thinking before a single screen is designed.
Desk research compressed from weeks to days.
Synthetic patient modelling replaces slow recruitment for quantitative depth.
Qualitative interview analysis surfaced faster, with fewer blind spots.
AI generates concept variants to accelerate creative divergence.
Options evaluated against defined criteria, not instinct.
Output: human strategy, reached faster and tested more rigorously.
AI-enhanced journeys
AI improves specific, existing steps without replacing the patient's role in them.
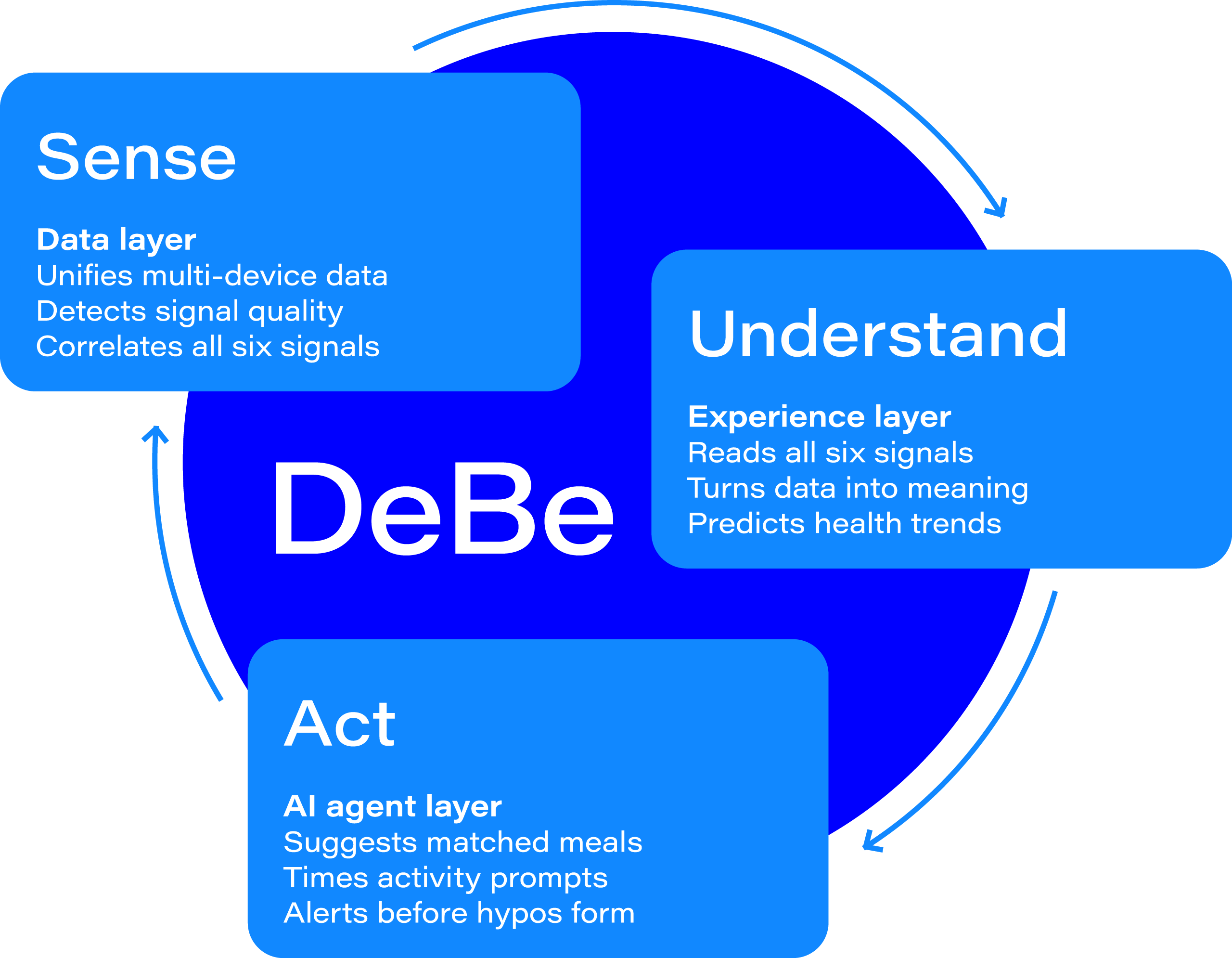
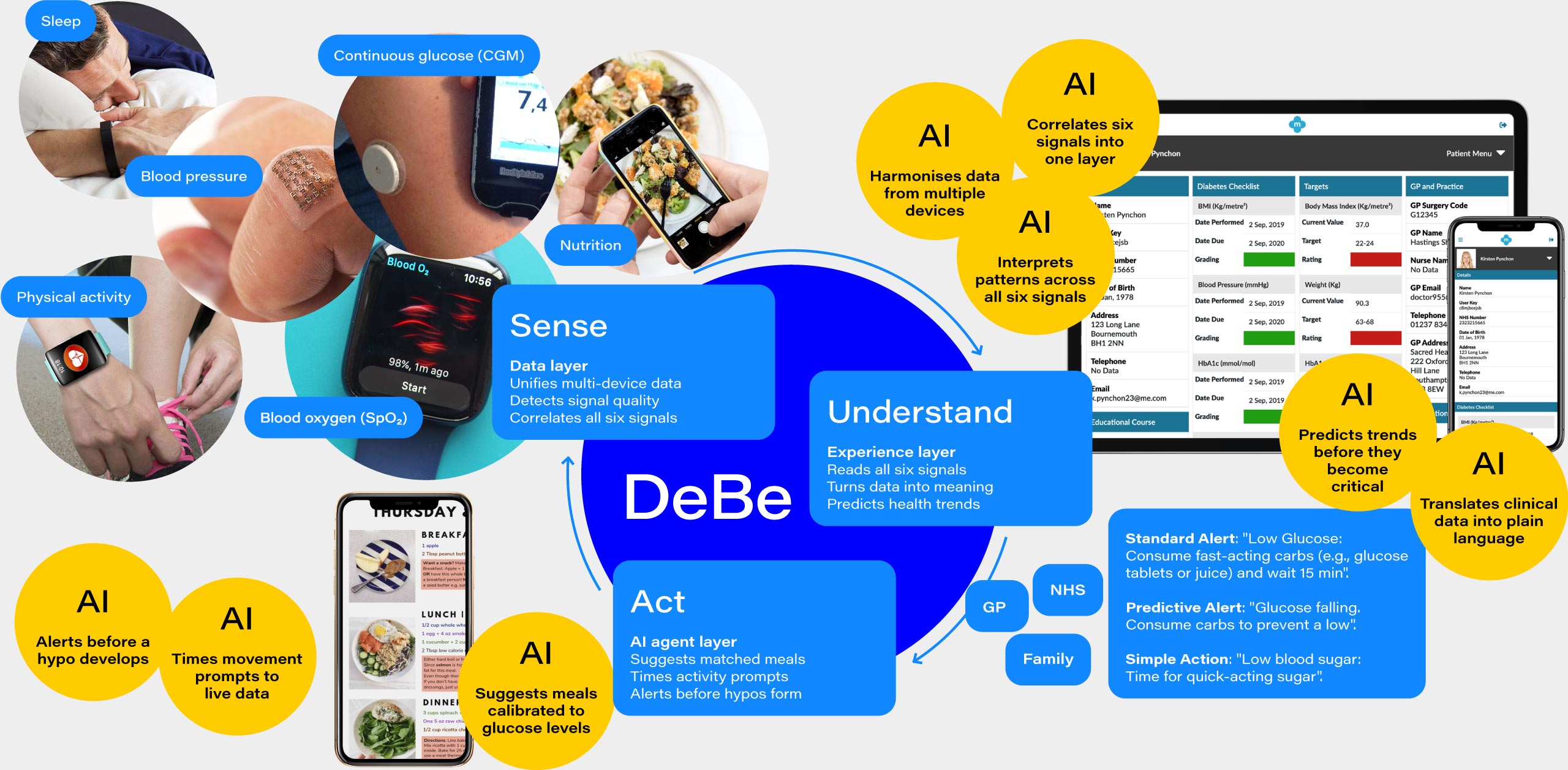
Sense: harmonises six signals, checks data quality, correlates in real time.
Understand: identifies daily, weekly, and longitudinal patterns; contextualises anomalies; translates clinical data into plain language.
Act: calibrates meal suggestions to live glucose; times movement prompts to trend data; fires alerts before symptoms appear.
AI-enabled journeys
AI acts. The patient stays in control.
Agents adjust shopping lists based on live meal plans and nutritional targets.
Clinical reports drafted automatically, pre-formatted for GP appointments.
Data summaries shared with NHS or family with patient consent.
Agent layer learns individual response patterns over time.
The 6 diabetes signals are: Continuous glucose (CGM), Blood pressure, Blood oxygen (SpO₂), Physical activity, Sleep, Nutrition.

System
AI is not a feature added to the system. It is the operating logic connecting three experience layers.
DeBe operates across three layers.
Sense is the device-agnostic data layer, integrating across CGMs, smartwatches, blood pressure monitors, oximeters, and fitness trackers via Apple HealthKit, Google Health Connect, and FHIR. No lock-in.
Understand is the experience layer. A mobile app for real-time awareness. A web interface for history, trends, and clinical sharing in plain language.
Act is the AI agent layer. Meal suggestions calibrated to live glucose levels. Movement prompts timed to trend data. Shopping list adjustments. Pre-formatted GP reports. Alerts before a hypo develops, not after symptoms appear.
The long-term ambition is to solve the interoperability problem at its root: open standards, shared data infrastructure, a system that works across every device a patient already owns.
DeBe senses your health signals, helps you understand what they mean, and acts with you to improve them.
Outcomes
A proposition in progress.
This project is in progress. The outcomes at this stage are methodological proof points, not commercial results.
Competitive gap confirmed and evidenced across peer-reviewed clinical literature, NIH/NIDDK research, and OECD health technology analysis.
Six-signal integration identified as the primary structural market gap: SpO₂ is absent from all existing patient-facing platforms.
Two behavioural segments defined with distinct onboarding strategies and one shared product architecture.
Regulatory compliance framework mapped across GDPR, AI Act, EAA, and DSA/DMA.
Four-phase go-to-market roadmap: Understand and Define → Prototype and Validate → Ship and Learn → Scale and Evolve.
DeBe is open to conversations
With investors, clinical partners, and health technology collaborators who share the belief that diabetes management needs a radically different approach.

Client: Self-initiated
Sectors: Digital Health, Healthcare, Consumer Technology
Role: Founder
Scope: Create - Product, Experience (CX, Service Design, BX)
Curious how this approach might apply in your context?
Call me Ale